-- Landmark ZUMA-7 Study was Initiated in 2017 as the First Randomized Clinical Trial to Test the Earlier Use of a CAR T-cell Therapy Against Standard of Care --
-- Study Met the Primary and Key Secondary Endpoints of Event-Free Survival and Objective Response Rate, Demonstrating a Highly Statistically and Clinically Significant Improvement Compared to Standard of Care --
Kite, a Gilead Company (Nasdaq: GILD), today announced top-line results from the primary analysis of ZUMA-7, a randomized Phase 3 global, multicenter study showing superiority of Yescarta® (axicabtagene ciloleucel) compared to standard of care (SOC) in second-line relapsed or refractory large B-cell lymphoma (LBCL). With a median follow-up of two years, the study met the primary endpoint of event-free survival (EFS; hazard ratio 0.398, p <0.0001). The study also met the key secondary endpoint of objective response rate (ORR). The interim analysis of overall survival (OS) showed a trend favoring Yescarta; however, the data are immature at this time, and further analyses are planned for the future.
This press release features multimedia. View the full release here: https://www.businesswire.com/news/home/20210628005449/en/
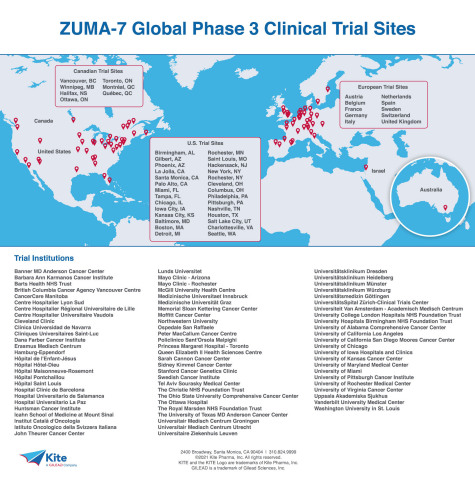
Kite Pharma ZUMA-7 Global Clinical Trial Sites Map - Centers
Overall survival measures deaths over time from any cause. Event-free survival is defined as time from randomization to disease progression, commencement of new lymphoma therapy, or death from any cause. ZUMA-7 was conducted under a Special Protocol Agreement (SPA) with the U.S. Food and Drug Administration (FDA) whereby the trial design, clinical endpoints and statistical analysis were agreed in advance with the Agency.
Safety results from the study were consistent with or lower than the known safety profile of Yescarta for the treatment of LBCL in the third-line setting. Six percent of patients experienced cytokine release syndrome (CRS) Grade 3 or higher, with a median onset of three days, and 21% experienced neurological events Grade 3 or higher. No new safety concerns were identified in this second-line setting.
“The top-line results of the randomized ZUMA-7 trial paint the picture of a potential paradigm shift in the treatment of large B-cell lymphoma,” said Frederick L. Locke, MD, ZUMA-7 Lead Principal Investigator and Co-Leader of the Immuno-Oncology Program at Moffitt Cancer Center, Tampa, Florida. “The outcomes for patients relapsing after frontline chemotherapy in this study are dramatically improved with rapid referral (to a CAR T center) and a single infusion of axicabtagene ciloleucel as compared to chemotherapy and consolidative autologous transplant, the longstanding second-line standard of care.”
ZUMA-7 evaluated an one-time infusion of the CAR T-cell therapy Yescarta compared to SOC in adult patients with relapsed or refractory LBCL. Standard of care for relapsed or refractory LBCL is a two-step process: immunochemotherapy is reintroduced, and if the patient responds and can tolerate further treatment, they move on to high-dose chemotherapy plus stem cell transplant.
“Yescarta has been instrumental in transforming outcomes for patients with third-line LBCL. Our goal has always been to bring the benefit of CAR T-cell therapy to more patients, earlier in their treatment, where the potential for benefit may be even greater,” said Christi Shaw, Chief Executive Officer of Kite. “As the leader in cell therapy, Kite is honored to deliver this landmark study and would like to thank the patients, families, physicians and care teams around the world that made this possible.”
ZUMA-7 was initiated in 2017 and enrolled 359 patients in 77 centers around the world. Results released today represent the longest follow-up time of any study in this setting with two years median follow-up. Patients enrolled in the study ranged in age from 22 to 81, with 30% of the patients 65 or older.
“Over 40 years ago, we learned the important role T-cells play in fighting cancer, and 20 years ago autologous stem cell transplant became an option to treat lymphoma. Today's results show us the potential power of cell therapy for patients with lymphoma when used earlier, and instead of standard treatment options,” said Frank Neumann, MD, PhD, Kite’s Global Head of Clinical Development.
Detailed results from ZUMA-7 will be submitted for presentation at a future medical congress, and Kite plans to initiate discussions with the U.S. Food and Drug Administration, European Medicines Agency and other global health authorities regarding submission of a supplemental Biologics License Application later this year to expand the currently approved indications for Yescarta. See About Yescarta section for current Yescarta approved indications. Yescarta has not been approved by any regulatory agency for the treatment of patients in the second-line setting similar to those in ZUMA-7.
About 40% of patients with LBCL will need second-line treatment, as their cancer will either relapse (return) or become refractory (not respond) to treatment.
About ZUMA-7 Study Design
ZUMA-7 is a randomized, open-label, global, multicenter, Phase 3 study evaluating the safety and efficacy of Yescarta versus current standard of care (SOC) for second-line therapy (platinum-based salvage combination chemotherapy regimen followed by high-dose therapy and autologous stem cell transplant in those who respond to salvage chemotherapy) in adult patients with relapsed or refractory (within or equal to 12 months of first-line therapy), large B-cell lymphoma (LBCL). In the study, 359 patients were randomized (1:1) to receive a single infusion of Yescarta or current SOC second-line therapy. The primary endpoint is event-free survival (EFS), defined as the time from randomization to the earliest date of disease progression per Lugano Classification (Cheson et al, 2014), commencement of new lymphoma therapy, or death from any cause as determined by blinded central review. Key secondary endpoints include objective response rate (ORR) and overall survival (OS). Other secondary endpoints include modified EFS, progression-free survival (PFS) and duration of response (DOR).
About Yescarta
Yescarta is a CD19-directed genetically modified autologous T cell immunotherapy indicated for the treatment of:
- Adult patients with relapsed or refractory large B-cell lymphoma after two or more lines of systemic therapy, including diffuse large B-cell lymphoma (DLBCL) not otherwise specified, primary mediastinal large B-cell lymphoma, high grade B-cell lymphoma, and DLBCL arising from follicular lymphoma. Limitations of Use: Yescarta is not indicated for the treatment of patients with primary central nervous system lymphoma.
- Adult patients with relapsed or refractory follicular lymphoma (FL) after two or more lines of systemic therapy. This indication is approved under accelerated approval based on response rate. Continued approval for this indication may be contingent upon verification and description of clinical benefit in confirmatory trial(s).
U.S. IMPORTANT SAFETY INFORMATION
BOXED WARNING: CYTOKINE RELEASE SYNDROME AND NEUROLOGIC TOXICITIES
- Cytokine Release Syndrome (CRS), including fatal or life-threatening reactions, occurred in patients receiving Yescarta. Do not administer Yescarta to patients with active infection or inflammatory disorders. Treat severe or life-threatening CRS with tocilizumab or tocilizumab and corticosteroids.
- Neurologic toxicities, including fatal or life-threatening reactions, occurred in patients receiving Yescarta, including concurrently with CRS or after CRS resolution. Monitor for neurologic toxicities after treatment with Yescarta. Provide supportive care and/or corticosteroids as needed.
- Yescarta is available only through a restricted program under a Risk Evaluation and Mitigation Strategy (REMS) called the Yescarta and Tecartus REMS Program.
CYTOKINE RELEASE SYNDROME (CRS), including fatal or life-threatening reactions, occurred. CRS occurred in 88% (224/254) of all patients with non-Hodgkin lymphoma (NHL), including Grade ≥3 in 10%. CRS occurred in 94% (101/108) of patients with large B-cell lymphoma (LBCL), including Grade ≥3 in 13%. Among patients with LBCL who died after receiving Yescarta, 4 had ongoing CRS events at the time of death. The median time to onset of CRS was 2 days (range: 1-12 days) and the median duration was 7 days (range: 2-58 days) for patients with LBCL. CRS occurred in 84% (123/146) of patients with indolent non-Hodgkin lymphoma (iNHL), including Grade ≥3 in 8% (11/146). Among patients with iNHL who died after receiving Yescarta, 1 patient had an ongoing CRS event at the time of death. The median time to onset of CRS was 4 days (range: 1-20 days) and median duration was 6 days (range: 1-27 days) for patients with iNHL. Key manifestations of CRS (≥10%) in all patients combined included fever (80%), hypotension (38%), tachycardia (29%), hypoxia (21%), chills (21%), and headache (13%). Serious events that may be associated with CRS include cardiac arrhythmias (including atrial fibrillation and ventricular tachycardia), cardiac arrest, cardiac failure, renal insufficiency, capillary leak syndrome, hypotension, hypoxia, multi-organ failure and hemophagocytic lymphohistiocytosis/macrophage activation syndrome. In a subsequent cohort of LBCL patients, tocilizumab and/or corticosteroids were administered for ongoing Grade 1 events. CRS occurred in 93% (38/41) of these patients and 2% (1/41) had Grade 3 CRS, with no patients experiencing a Grade 4 or 5 event. The median time to onset of CRS was 2 days (range: 1 to 8 days) and the median duration of CRS was 7 days (range: 2 to 16 days). Key manifestations of CRS (>5%) included pyrexia, hypotension, chills, headache, nausea, tachycardia, C-reactive protein increased, fatigue, hypoxia, and vomiting. Ensure that 2 doses of tocilizumab are available prior to Yescarta infusion. Following infusion, monitor patients for signs and symptoms of CRS at least daily for 7 days at the certified healthcare facility, and for 4 weeks thereafter. Counsel patients to seek immediate medical attention should signs or symptoms of CRS occur at any time. At the first sign of CRS, institute treatment with supportive care, tocilizumab, or tocilizumab and corticosteroids as indicated.
NEUROLOGIC TOXICITIES that were fatal or life-threatening occurred. Neurologic toxicities occurred in 81% (206/254) of all patients with NHL receiving Yescarta, including Grade ≥3 in 26%. Neurologic toxicities occurred in 87% (94/108) of patients with LBCL, including Grade ≥3 in 31%. The median time to onset was 4 days (range: 1-43 days) and the median duration was 17 days for patients with LBCL. Neurologic toxicities occurred in 77% (112/146) of patients with iNHL, including Grade ≥3 in 21%. The median time to onset was 6 days (range: 1-79 days) and the median duration was 16 days for patients with iNHL. 98% of all neurologic toxicities in patients with LBCL and 99% of all neurologic toxicities in patients with iNHL occurred within the first 8 weeks of Yescarta infusion. Neurologic toxicities occurred within the first 7 days of infusion for 89% of affected patients with LBCL and 74% of affected patients with iNHL. The most common neurologic toxicities (≥10%) in all patients combined included encephalopathy (53%), headache (45%), tremor (31%), dizziness (20%), delirium (16%), aphasia (15%), and insomnia (11%). Prolonged encephalopathy lasting up to 173 days was noted. Serious events, including leukoencephalopathy and seizures, as well as fatal and serious cases of cerebral edema, have occurred. In a subsequent cohort of LBCL patients who received corticosteroids at the onset of Grade 1 toxicities, neurologic toxicities occurred in 78% (32/41) of these patients and 20% (8/41) had Grade 3 neurologic toxicities with no patients experiencing a Grade 4 or 5 event. The median time to onset of neurologic toxicities was 6 days (range: 1-93 days) with a median duration of 8 days (range: 1-144 days). The most common neurologic toxicities were consistent with the overall LBCL population treated with Yescarta. Following Yescarta infusion, monitor patients for signs and symptoms of neurologic toxicities at least daily for 7 days at the certified healthcare facility, and for 4 weeks thereafter, and treat promptly.
REMS: Because of the risk of CRS and neurologic toxicities, Yescarta is available only through a restricted program called the Yescarta and Tecartus REMS Program which requires that: Healthcare facilities that dispense and administer Yescarta must be enrolled and comply with the REMS requirements and must have on-site, immediate access to a minimum of 2 doses of tocilizumab for each patient for infusion within 2 hours after Yescarta infusion, if needed for treatment of CRS. Certified healthcare facilities must ensure that healthcare providers who prescribe, dispense, or administer Yescarta are trained about the management of CRS and neurologic toxicities. Further information is available at www.YescartaTecartusREMS.com or 1-844-454-KITE (5483).
HYPERSENSITIVITY REACTIONS: Allergic reactions, including serious hypersensitivity reactions or anaphylaxis, may occur with the infusion of Yescarta.
SERIOUS INFECTIONS: Severe or life-threatening infections occurred. Infections (all grades) occurred in 47% (119/254) of all patients with NHL. Grade ≥3 infections occurred in 19% of patients, Grade ≥3 infections with an unspecified pathogen occurred in 15%, bacterial infections in 5%, viral infections in 2%, and fungal infections in 1%. Yescarta should not be administered to patients with clinically significant active systemic infections. Monitor patients for signs and symptoms of infection before and after infusion and treat appropriately. Administer prophylactic anti-microbials according to local guidelines. Febrile neutropenia was observed in 40% of all patients with NHL and may be concurrent with CRS. In the event of febrile neutropenia, evaluate for infection and manage with broad-spectrum antibiotics, fluids, and other supportive care as medically indicated. In immunosuppressed patients, including those who have received Yescarta, life-threatening and fatal opportunistic infections including disseminated fungal infections (e.g., candida sepsis and aspergillus infections) and viral reactivation (e.g., human herpes virus-6 [HHV-6] encephalitis and JC virus progressive multifocal leukoencephalopathy [PML]) have been reported. The possibility of HHV-6 encephalitis and PML should be considered in immunosuppressed patients with neurologic events and appropriate diagnostic evaluations should be performed. Hepatitis B virus (HBV) reactivation, in some cases resulting in fulminant hepatitis, hepatic failure, and death, can occur in patients treated with drugs directed against B cells. Perform screening for HBV, HCV, and HIV in accordance with clinical guidelines before collection of cells for manufacturing.
PROLONGED CYTOPENIAS: Patients may exhibit cytopenias for several weeks following lymphodepleting chemotherapy and Yescarta infusion. Grade ≥3 cytopenias not resolved by Day 30 following Yescarta infusion occurred in 30% of all patients with NHL and included neutropenia (22%), thrombocytopenia (13%), and anemia (5%). Monitor blood counts after infusion.
HYPOGAMMAGLOBULINEMIA and B-cell aplasia can occur. Hypogammaglobulinemia occurred in 17% of all patients with NHL. Monitor immunoglobulin levels after treatment and manage using infection precautions, antibiotic prophylaxis, and immunoglobulin replacement. The safety of immunization with live viral vaccines during or following Yescarta treatment has not been studied. Vaccination with live virus vaccines is not recommended for at least 6 weeks prior to the start of lymphodepleting chemotherapy, during Yescarta treatment, and until immune recovery following treatment.
SECONDARY MALIGNANCIES may develop. Monitor life-long for secondary malignancies. In the event that one occurs, contact Kite at 1-844-454-KITE (5483) to obtain instructions on patient samples to collect for testing.
EFFECTS ON ABILITY TO DRIVE AND USE MACHINES: Due to the potential for neurologic events, including altered mental status or seizures, patients are at risk for altered or decreased consciousness or coordination in the 8 weeks following Yescarta infusion. Advise patients to refrain from driving and engaging in hazardous occupations or activities, such as operating heavy or potentially dangerous machinery, during this initial period.
ADVERSE REACTIONS: The most common adverse reactions (incidence ≥20%) in patients with LBCL included CRS, fever, hypotension, encephalopathy, tachycardia, fatigue, headache, decreased appetite, chills, diarrhea, febrile neutropenia, infections with pathogen unspecified, nausea, hypoxia, tremor, cough, vomiting, dizziness, constipation, and cardiac arrhythmias. The most common non-laboratory adverse reactions (incidence ≥20%) in patients with iNHL included fever, CRS, hypotension, encephalopathy, fatigue, headache, infections with pathogen unspecified, tachycardia, febrile neutropenia, musculoskeletal pain, nausea, tremor, chills, diarrhea, constipation, decreased appetite, cough, vomiting, hypoxia, arrhythmia, and dizziness.
Please see full Prescribing Information, including BOXED WARNING and Medication Guide.
About Kite
Kite, a Gilead Company, is a global biopharmaceutical company based in Santa Monica, California, with commercial manufacturing operations in North America and Europe. Kite’s singular focus is cell therapy to treat and potentially cure cancer. As the cell therapy leader, Kite has more approved CAR T indications to help more patients than any other company. For more information on Kite, please visit www.kitepharma.com.
About Gilead Sciences
Gilead Sciences, Inc. is a biopharmaceutical company that has pursued and achieved breakthroughs in medicine for more than three decades, with the goal of creating a healthier world for all people. The company is committed to advancing innovative medicines to prevent and treat life-threatening diseases, including HIV, viral hepatitis and cancer. Gilead operates in more than 35 countries worldwide, with headquarters in Foster City, California.
Forward-Looking Statements
This press release includes forward-looking statements within the meaning of the Private Securities Litigation Reform Act of 1995 that are subject to risks, uncertainties and other factors, including the possibility of unfavorable results from ongoing and additional clinical trials involving Yescarta. These and other risks, uncertainties and other factors are described in detail in Gilead’s Quarterly Report on Form 10-Q for the quarter ended March 31, 2021, as filed with the U.S. Securities and Exchange Commission. These risks, uncertainties and other factors could cause actual results to differ materially from those referred to in the forward-looking statements. All statements other than statements of historical fact are statements that could be deemed forward-looking statements. Investors are cautioned that any such forward-looking statements are not guarantees of future performance and involve risks and uncertainties and are cautioned not to place undue reliance on these forward-looking statements. All forward-looking statements are based on information currently available to Kite and Gilead, and Kite and Gilead assume no obligation and disclaim any intent to update any such forward-looking statements.
U.S. Prescribing Information for Yescarta including BOXED WARNING, is available at www.kitepharma.com and www.gilead.com.
Kite, the Kite logo, Yescarta, Tecartus, XLP and GILEAD are trademarks of Gilead Sciences, Inc. or its related companies.
For more information on Kite, please visit the company’s website at www.kitepharma.com or call Gilead Public Affairs at 1-800-GILEAD-5 or 1-650-574-3000. Follow Kite on social media on Twitter (@KitePharma) and LinkedIn.
View source version on businesswire.com: https://www.businesswire.com/news/home/20210628005449/en/
Contacts
Jacquie Ross, Investors
(650) 358-1054
Mary Lynn Carver, Media
(410) 443-1853